Quick Summary: Molluscum contagiosum causes distinct, pearly skin bumps that usually go away on their own. While often harmless, these viral lesions can spread easily through touch.
- The condition typically resolves within 6 to 24 months without medical intervention.
- Treatment options range from watchful waiting to procedures like cryotherapy or topical agents.
- Avoiding scratching is crucial to prevent spreading the virus to other body parts.
- Immunocompromised individuals require more aggressive management strategies.
- School exclusion is generally unnecessary; focus instead on hygiene and covering lesions.
What Exactly Are These Pearly Bumps?
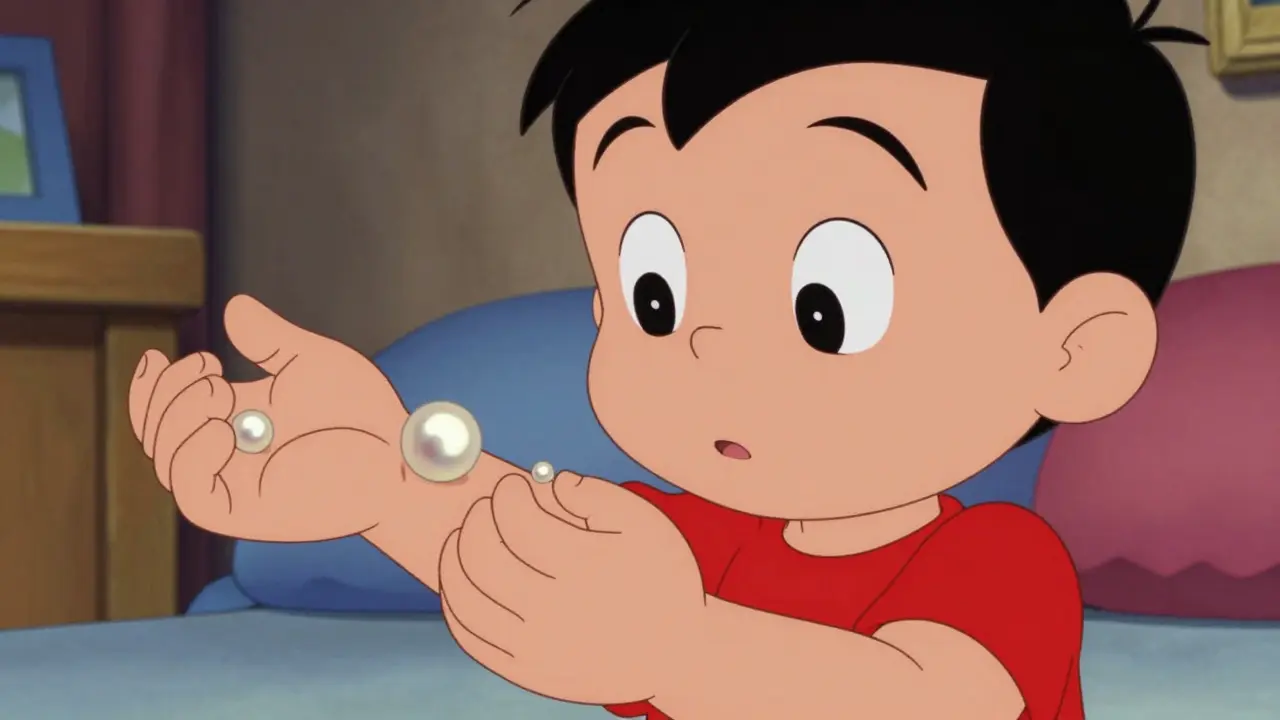
You might spot strange bumps on your child's arm or torso and wonder if they are something serious. Often, these are signs of Molluscum Contagiosum, a viral skin infection characterized by small, raised lesions. In our clinics here in Edinburgh, parents frequently worry these are insect bites or warts, but the presentation is actually quite specific. Unlike standard rashes, you will notice firm, dome-shaped papules that have a tiny dimple or depression right in the center. This feature, known medically as umbilication, is the hallmark of the condition.
The size of these bumps varies significantly depending on the person's immune health. For most children and healthy adults, the lesions stay small, ranging from a pinhead size (about 2 millimeters) up to the size of a pencil eraser (roughly 6 millimeters). They often appear white, pink, or skin-colored, sometimes with a shiny, pearly quality. We see them mostly on the face, trunk, arms, and legs. Interestingly, they rarely show up on the palms of the hands or soles of the feet, which helps distinguish them from other dermatological issues.
Understanding the Virus Behind the Rashes
The culprit behind these bumps is the Molluscum Contagiosum Virus, a member of the poxvirus family that infects the top layers of the skin. It's important to understand that this is a specific type of pathogen called Muscillopoxvirus. Once the virus enters the skin cells, it replicates rapidly, causing the characteristic swelling you see. The incubation period-the time between exposure and seeing symptoms-usually takes anywhere from two to six weeks. During this window, a person could unknowingly pass it on because nothing is visible yet.
While we often associate viruses with cold seasons, this particular strain thrives in warm, humid environments. If you live near coastal areas where humidity is higher, or if you spend a lot of time in pools or locker rooms, transmission rates increase. The virus survives well on surfaces, meaning towels, clothes, and even pool toys can act as vectors for spreading the infection to others.

How Does It Spread in Daily Life?
Transmission happens through direct contact. Think about how families interact during playtime or sports practice. Skin-to-skin friction allows the virus to jump from one person to another. For example, wrestling in a playground game can transfer the virus from an infected area on one child to the uninfected skin of another. Household studies suggest that sharing towels alone can reduce household spread by roughly 57% if avoided, highlighting the role of fomites.
In swimming pools, the water itself isn't the main carrier, but the wet environment softens the skin, making entry easier for the virus. Many gyms and schools have policies now recommending that lesions be covered with waterproof bandages during activities. Scratching is a major accelerator of spread too. When someone scratches an itch caused by the lesions, the fluid containing the virus transfers to their fingertips and subsequently to wherever else they touch, potentially increasing lesion counts by up to 300% on average across the body.
Active Treatments versus Watchful Waiting
When you walk into a clinic, the first question is always "do I need to treat this?" Medical consensus from major groups like the American Academy of Dermatology leans heavily toward observation for immunocompetent patients. Why rush to intervene when the body fights it off naturally? About 92% of cases resolve completely within 18 months without scarring. For many parents, doing nothing is the safest bet to avoid discomfort and unnecessary costs.
However, there are valid reasons to consider active treatment. If the lesions are on the face and causing social anxiety or bullying, removing them early makes sense. We also consider active removal if the patient has severe eczema, as the itching creates a cycle of re-infection. Below is a comparison of common methods used when treatment becomes necessary:
| Treatment Method | ||||
|---|---|---|---|---|
| Procedure Name | Success Rate | Pain Level | Scarring Risk | Availability |
| Cryotherapy (Freezing) | Moderate | High | Low to Moderate | Widely Available |
| Cantharidin | High (73%) | Moderate | Low | Clinic Only |
| Potassium Hydroxide | Moderate | Mild | Very Low | Compounded Cream |
Cantharidin stands out as a blistering agent applied by professionals. It works by peeling the skin around the bump, essentially popping the roof off the lesion so the immune system can clear the debris. Studies indicate it clears lesions effectively compared to placebo, but it requires multiple visits over several weeks. Another option involves potassium hydroxide creams, often available over the counter or compounded. These chemically dissolve the virus particles over time. While effective, consistency matters-you have to apply it daily for weeks to see a result.
Navigating Complications and High-Risk Groups
For the vast majority of healthy individuals, this is a nuisance, not a threat. But the landscape changes entirely for immunocompromised patients. If you or a loved one has HIV/AIDS, particularly with low CD4 counts, these lesions can behave differently. Instead of resolving, they can become widespread and massive, sometimes exceeding 3 centimeters in diameter. In these cases, watchful waiting fails, and aggressive management including optimizing antiretroviral therapy is critical.
We also see a strong link between molluscum and Atopic Dermatitis, commonly known as eczema. Children with compromised skin barriers due to eczema have a much harder time fighting off the virus. Their inflamed skin provides a better foothold for the infection, leading to faster spread and more intense itching. Managing the eczema itself often helps control the molluscum flare-up, breaking the itch-scratch-infect cycle that keeps the condition alive.
Frequently Asked Questions
Is Molluscum Contagiosum contagious to adults?
Yes, adults can contract the virus, often through sexual contact or close physical interaction with infected children. While less common in adults than children, it remains highly transmissible via skin contact.
Should my child stop going to school?
Current guidelines state that children should not be excluded from school solely for having molluscum. Encouraging good hygiene and keeping lesions covered during swimming is sufficient to manage risk.
Will these bumps leave scars?
Usually not. Most lesions fade away without a trace. However, aggressive treatments like freezing or picking at the bumps can cause permanent scarring or pigment changes.
How long does it take to heal naturally?
Natural resolution typically occurs within 6 to 12 months, but it can take up to 24 months in some cases. Individual variation depends largely on immune response strength.
Can I swim with molluscum contagiosum?
Swimming is permitted provided lesions are covered with waterproof dressings. Uncovered lesions pose a contamination risk to the pool water and other swimmers.
tyler lamarre
March 29, 2026 AT 01:58It is frankly amusing that people rush to cryotherapy when watchful waiting is objectively superior.
Most dermatologists simply want billable procedures to maintain their practice revenue stream.
The immune system clears this poxvirus without significant intervention in the vast majority of cases anyway.
Scarring risks associated with aggressive removal vastly outweigh the temporary aesthetic concern of bumps.
Parents often panic because they lack basic virological literacy regarding common childhood conditions.
They prioritize speed over biological wisdom.
The umbilication feature is a clear diagnostic sign that requires no chemical dissolution.
Applying cantharidin causes unnecessary inflammation during the healing process.
Why introduce caustic agents when the body already possesses the tools?
This viral infection behaves much better under observation than under the microscope of treatment.
Lesions resolve themselves faster than most patients anticipate once the anxiety subsides.
The social pressure drives demand rather than medical necessity.
We see far too much harm done by trying to fix something that fixes itself naturally.
Medical consensus is often skewed by economic incentives rather than patient outcomes.
Patience remains the most effective tool in any pediatric clinic arsenal today.
Paul Vanderheiden
March 29, 2026 AT 16:13totally agree with the take on watchful waiting being best
stress usually makes the skin act up worse anyway
letting the kid be a kid while it heals is important too
Tony Yorke
March 31, 2026 AT 03:29Just let it ride and cover the lesions.
kendra 0712
April 1, 2026 AT 23:06THIS IS SO IMPORTANT FOR PARENTS TO KNOW!!!
You literally save your family from so much mess if you just cover the bumps!!
Swimming pools can get really contaminated if you ignore this!
Please teach your kids to stop scratching!!!!
It spreads so fast otherwise!!!
I learned this the hard way last summer!!!
Stay safe out there!!!
Rachael Hammond
April 3, 2026 AT 17:54my son had thier for a while last year and we learned so much abt hygiene becuse his eczema made it worse
covering the spots was key to keeping it from spreding around the house
i think the part about scraching causing more bumps is really spot on
we tried to stop him from touching his face all the time
it helps to remind him gently without making him feel bad about his skin
the bumps did go away eventually even though we wanted them gone sooner
Poppy Jackson
April 4, 2026 AT 15:00oh dear that sounds so stressful for everyone involved
poor little thing dealing with all that worry and itching
hopefully time will heal it all properly for him
Jordan Marx
April 6, 2026 AT 01:28From a clinical standpoint the pathophysiology involves the epidermal hyperplasia induced by the virus
Transmission vectors include fomites which necessitates strict barrier precautions during aquatic activities
Immunocompetence plays a pivotal role in lesion clearance rates observed longitudinally
Cryotherapy induces cellular necrosis through thermal damage mechanisms which carries inherent risk profiles
Topical retinoids might offer an alternative mechanism of action for those hesitant about freezing
We must consider the psychological burden placed on the developing psyche of a school age child
Social stigmatization occurs despite the benign nature of the underlying pathology
Management strategies should always prioritize evidence-based guidelines over anecdotal fear
Monitoring the progression allows for accurate assessment of the host immune response
Delayed resolution in certain populations indicates a deeper systemic issue requiring investigation
The presence of co-morbid atopic dermatitis exacerbates the inflammatory cascade significantly
Treating the underlying barrier defect often resolves the secondary infection concurrently
Intervention thresholds should be personalized to patient comfort and family dynamics
Standardizing care prevents unnecessary medicalization of self-limiting conditions entirely
We see improved compliance when families understand the natural history thoroughly
Jeannette Kwiatkowski Kwiatkowski
April 6, 2026 AT 08:24your jargon heavy talk is actually quite annoying to normal people reading this
its nice to see someone who knows the science but dont confuse us
less fancy words please and more real world advice
i guess some of it is useful for understanding severity
Aaron Olney
April 6, 2026 AT 16:50OMG this hits hard cause my nephew got it everywhere after one campout
it was such a drama and mom was crying thinking it was something evil
the doc said nothing to do but wait but she kept buying creams
now he looks fine but scars from the freezing thing are still there
why take risks?? the water stuff is scarry though if you love swimming
just dont scratch and cover them up please guys
its contagious so dont share towels ever
Kameron Hacker
April 7, 2026 AT 04:12Public health guidelines often fail to address the nuances of individual transmission rates adequately
Parents must be educated on the distinction between contagion and infection pathways clearly
School policies vary widely regarding exclusion criteria which creates confusion
Medical professionals need to assert authority when parents demand aggressive cosmetic intervention unnecessarily
The data supports conservative management yet cultural expectations push for immediate action
This discrepancy highlights a failure in patient education regarding viral life cycles
Compliance improves when consequences of non-compliance are stated firmly during consultation
Sophie Hallam
April 7, 2026 AT 22:47communication styles vary a lot across different clinics
finding a middle ground works best for families usually