Statin Interaction Checker
Check Your Statin Interactions
Select your statin and any other medications you're taking to assess muscle pain risk.
Interaction Result
Statins save lives. They cut heart attack and stroke risk in half for people with high cholesterol or a history of cardiovascular disease. But for some, the benefit comes with a painful trade-off: muscle pain, weakness, or worse. This isn’t just a side effect-it’s a real, measurable risk called myopathy. And it’s often not the statin alone that causes it. It’s what you’re taking alongside it.
What Exactly Is Statin-Induced Myopathy?
Myopathy means your muscles aren’t working right. It’s not just soreness after a workout. True statin-induced myopathy shows up as unexplained muscle pain, cramps, or weakness. You might feel it in your thighs, shoulders, or even when climbing stairs. In rare cases, it escalates to rhabdomyolysis-where muscle fibers break down and leak into your bloodstream, risking kidney failure. This is life-threatening, but it’s extremely rare: less than 1 in 10,000 people on statins.
The real danger isn’t the statin itself. It’s the combination. Some medications you’re already taking can push statin levels in your blood dangerously high. And once those levels rise, your muscles pay the price.
Not All Statins Are Created Equal
There are six main statins used today. But they’re not all the same when it comes to muscle risk. The difference comes down to how they’re processed in your body.
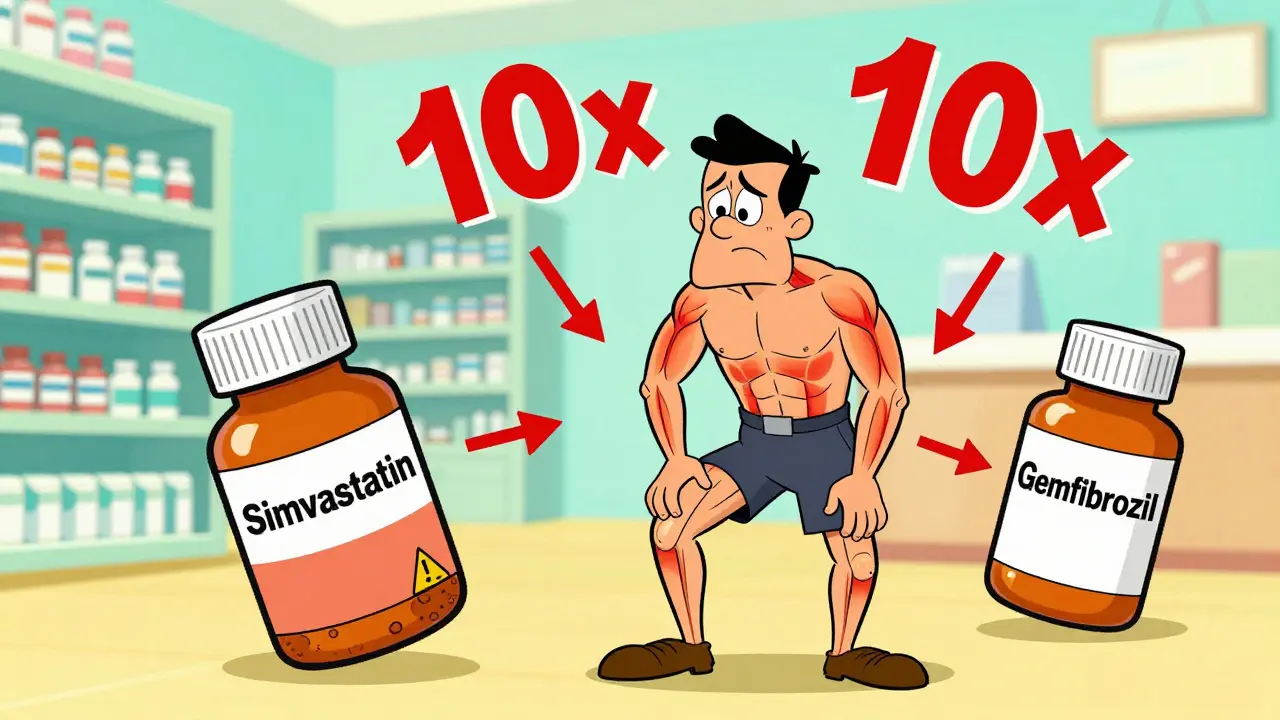
Statins like simvastatin, lovastatin, and atorvastatin are broken down by a liver enzyme called CYP3A4. That’s fine-until you take something that blocks it. Macrolide antibiotics like clarithromycin and erythromycin do exactly that. When you combine them with simvastatin, your blood levels of the statin can spike by up to 10 times. That’s why the NHS recommends stopping simvastatin during a course of clarithromycin, even if it’s just for 7 days.
On the other end of the spectrum, pravastatin, rosuvastatin, and fluvastatin aren’t heavily processed by CYP3A4. They’re safer when paired with antibiotics. Pravastatin, in particular, has the lowest reported rate of muscle symptoms-just 0.6% to 1.4% of users. Rosuvastatin, despite being powerful, has a higher reported rate of muscle issues (up to 12.7%), but that’s more likely tied to dose than metabolism.
Here’s a quick breakdown:
| Statin | Primary Metabolism Pathway | Myopathy Risk | Interaction Risk with Macrolides |
|---|---|---|---|
| Simvastatin | CYP3A4 (95%) | High | Very High (up to 10x increase) |
| Lovastatin | CYP3A4 (95%) | High | Very High |
| Atorvastatin | CYP3A4 (70%) | Moderate | Moderate (up to 4x increase) |
| Pravastatin | Non-CYP3A4 | Low | Negligible |
| Rosuvastatin | Non-CYP3A4 | Moderate to High (dose-dependent) | Low |
| Fluvastatin | CYP2C9 | Low | Low |
These Medications Are the Real Culprits
It’s not just antibiotics. Many common drugs can turn a safe statin into a risky one.
- Cyclosporine (used after transplants) can increase statin levels by 3 to 13 times. Avoid combining it with simvastatin or lovastatin entirely.
- Gemfibrozil (a fibrate for triglycerides) increases statin levels by about 2-fold. It’s one of the worst offenders. Health Canada even added a black box warning for this combo. Fenofibrate is safer.
- Diltiazem and verapamil (blood pressure meds) inhibit the same liver pathways. The FDA now limits simvastatin to 20mg max if you’re on either of these.
- Amiodarone (for irregular heartbeat) also increases risk. Again, simvastatin 20mg is the max allowed.
- Azithromycin is an exception. Unlike clarithromycin or erythromycin, it doesn’t block CYP3A4. So if you need an antibiotic and are on a statin, ask for azithromycin.
It’s not just drugs. Age, body size, kidney function, and even exercise matter. People over 75, those with low body weight, or with hypothyroidism or kidney disease are at higher risk. Heavy exercise, especially if you’re not used to it, can also trigger muscle symptoms.
What Should You Do If You Have Muscle Pain?
Don’t assume it’s the statin. Muscle pain is common. It could be from aging, arthritis, or even vitamin D deficiency. But if you started a new medication or changed your statin dose around the same time, it’s worth investigating.
Here’s what to do:
- Check your meds. Make a list of everything you’re taking-including supplements. Share it with your doctor or pharmacist.
- Get a CK test. Creatine kinase is a muscle enzyme. If it’s more than 10 times the normal level, that’s a red flag for myopathy. If it’s 5 times higher and you have symptoms, your doctor may pause the statin.
- Don’t quit cold turkey. Stopping statins without a plan increases heart attack risk. Work with your provider to find a safer option.
Many people who think they’re statin-intolerant can actually tolerate a different statin. One study found that 71% of people who stopped statins due to muscle pain could go back on a different one at a lower dose.
What Are the Alternatives?
If you can’t tolerate statins, you’re not out of options.
- Switch to pravastatin or fluvastatin. These have the lowest interaction risk and are often well-tolerated.
- Try a lower dose. Sometimes, 10mg of atorvastatin or 5mg of rosuvastatin still lowers cholesterol enough-with far fewer side effects.
- Use bempedoic acid (Nexletol). This newer drug lowers LDL without entering muscle tissue. It’s not cheap-around $4,000 a year-but it’s an option for those who can’t take statins at all.
- Consider PCSK9 inhibitors. These are injectable drugs that slash LDL dramatically. They’re used for people with genetic cholesterol disorders or those who’ve had heart attacks despite statins.
- Try icosapent ethyl (Vascepa). This purified fish oil has been shown to reduce heart events in people already on statins. It’s not a replacement, but it can help reduce the need for high-dose statins.
Some doctors also suggest coenzyme Q10 (CoQ10) supplements-100 to 200mg daily. The science is mixed, but many patients report less muscle pain when taking it. It’s low-risk, so it’s worth a trial.
What’s New in 2026?
Genetic testing is slowly becoming part of the picture. A gene called SLCO1B1 affects how your body handles statins. People with a certain variant have a 4.5 times higher risk of myopathy from simvastatin. The FDA added this info to simvastatin’s label in 2011, but most doctors don’t test for it routinely-yet.
Another emerging idea is intermittent dosing. Instead of taking rosuvastatin daily, some patients take it every other day. Early trials suggest it works almost as well, with fewer muscle issues. Results from the 2023 DECLARE trial should be out by late 2024 or early 2025. If they’re positive, this could change how we prescribe statins for people at risk.
Bottom Line: Don’t Panic, But Do Be Smart
Statins are still the best tool we have to prevent heart attacks and strokes. The benefits far outweigh the risks for most people. But if you’re on one and you’re also taking another medication, you need to know the combo.
Ask your pharmacist: "Is my statin safe with my other meds?" If you’re on clarithromycin, diltiazem, or gemfibrozil, don’t guess-get a clear answer. If you feel unexplained muscle pain, don’t ignore it. Get your CK levels checked. And if you’ve stopped statins because of muscle pain, talk to your doctor before giving up on them forever. There’s almost always a way forward.
Can I take statins with antibiotics?
It depends on the antibiotic. Clarithromycin and erythromycin can dangerously raise statin levels-especially simvastatin and lovastatin. Avoid them together. Azithromycin is safe. Always check with your pharmacist before starting a new antibiotic if you take a statin.
Which statin has the lowest risk of muscle pain?
Pravastatin has the lowest reported rate of muscle symptoms-only 0.6% to 1.4% of users. Fluvastatin is also low-risk. Both are metabolized outside the CYP3A4 pathway, making them safer with other medications. Rosuvastatin and simvastatin have higher rates, especially at higher doses.
Should I get a blood test if I have muscle pain?
Yes. A creatine kinase (CK) test measures muscle damage. If your CK is over 10 times the normal level and you have symptoms, that confirms statin-induced myopathy. Even if it’s only 5 times higher, your doctor may pause your statin to see if symptoms improve.
Can I restart a statin after stopping due to muscle pain?
Yes, often. Studies show 71% of people who stopped statins because of muscle pain can tolerate a different statin at a lower dose. Switching from simvastatin to pravastatin is a common and successful strategy. Never stop without talking to your doctor first.
Are there statins that don’t cause muscle pain at all?
No statin is completely free of muscle risk, but some are much safer. Pravastatin and fluvastatin have the lowest rates. Bempedoic acid (Nexletol) doesn’t enter muscle tissue and causes far fewer muscle side effects. It’s not a statin, but it’s an option for people who can’t tolerate them.
Bridget Verwey
March 5, 2026 AT 03:46Okay but like... why is everyone still on simvastatin? Like I get it’s cheap but come on. My grandma was on it for 12 years, then got prescribed clarithromycin for a sinus infection and ended up in physical therapy for six months. She’s fine now on pravastatin. Just switch. It’s not that hard.
Andrew Poulin
March 5, 2026 AT 23:51Stop overcomplicating this. If you have muscle pain and are on a statin, it’s the statin. Get off it. Try a different one. If it still hurts, it’s not the statin. Done.
Weston Potgieter
March 6, 2026 AT 16:27Bro just take CoQ10 and chill. I’ve been on 80mg of atorvastatin for 5 years with zero issues. Everyone’s just scared of their own shadow. Also azithromycin is fine. I take it with my statin every time I get a cold. No big deal. My doctor says I’m fine. He’s a doctor. He knows.
Vikas Verma
March 7, 2026 AT 08:26From a clinical perspective, the CYP3A4-mediated interactions are well-documented. However, real-world adherence to pharmacist-led medication reconciliation remains suboptimal. I recommend structured medication reviews every 6 months, particularly in polypharmacy patients over 65. Pravastatin remains the gold standard for low-risk profiles.
Sean Callahan
March 8, 2026 AT 16:45i hate how people act like statins are this evil thing. i had a heart attack at 48. statins saved my life. yes i got muscle cramps. so what. i take magnesium. i stretch. i drink water. i dont quit because my legs feel weird. you think your body is gonna thank you for stopping your meds? lol
Jeff Mirisola
March 10, 2026 AT 13:25My uncle was told he couldn’t take statins because of muscle pain. He switched to fluvastatin 20mg. No issues. Went from 190 to 130 LDL. He’s hiking mountains now. Don’t give up on statins. Just find the right one. It’s not a one-size-fits-all world.
Ian Kiplagat
March 10, 2026 AT 17:29Pravastatin ftw. 🌿
Amina Aminkhuslen
March 12, 2026 AT 02:42Someone needs to make a chart with emojis. Like 🚫 for clarithromycin, ✅ for azithromycin, 🤕 for muscle pain, 🚑 for rhabdo. People get it better that way. Stop with the tables. No one reads them.
amber carrillo
March 12, 2026 AT 10:09I appreciate how thorough this post is. Many people don’t realize how many common medications can interact. I always encourage patients to bring a full list of supplements to their appointments. Even herbal teas can matter.
Tim Hnatko
March 13, 2026 AT 17:43I’ve been a pharmacist for 18 years. The most common mistake? Patients don’t tell their doctors about OTC meds. I’ve seen people take ibuprofen daily with simvastatin and wonder why their CK is sky-high. It’s not the statin. It’s the combo. Always ask your pharmacist. They’re not just the people who hand out pills.
Aaron Pace
March 14, 2026 AT 22:33bro i just took azithromycin and simva together and my legs felt weird for 2 days 😅
Joey Pearson
March 15, 2026 AT 06:56My mom tried bempedoic acid. Cost her $300/month. But her LDL dropped 50%. She’s happier now. I wish insurance covered it better. Still, if you can’t tolerate statins, it’s a real lifeline. Don’t let price scare you off. Talk to your doc about patient assistance programs.